
People with diabetes are unfortunately at a higher risk for numerous ocular complications, which can lead to severe vision loss and sometimes even blindness. One of those eye diseases is diabetic retinopathy, the leading cause of blindness among Americans.
Diabetic retinopathy is an eye disease that damages the blood vessels in the retina. While what exactly causes this damage is not known, poorly controlled blood sugar levels are believed to be a contributing factor. Although diabetic retinopathy can affect persons with Type I or Type II diabetes, persons with Type I diabetes are at a greater risk of developing the disease. Over time, the risk of developing diabetic retinopathy increases.
TYPES OF DIABETIC RETINOPATHY
There are two main categories of diabetic retinopathy:
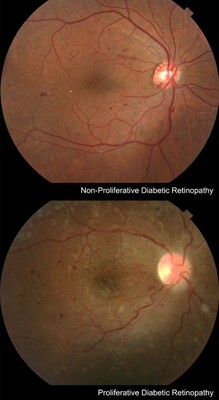
Non-proliferative: The small blood vessels in the retina become damaged and can leak fluid into the retinal tissue. This is called macular edema, which is swelling of the retina in the area that serves central vision. Symptoms of macula edema include blurry vision and loss of portions of the field of vision.
Proliferative: Newly formed abnormal blood vessels develop along the surface of the retina and are very fragile. Their fragility can cause them to bleed, which can cause severe vision loss and even blindness.
As these vessels proliferate, bleed and subsequently scar, they can detach the retina. These forms of retinal detachment pose unique challenges for the retinal surgeon.
Another complication is the obstruction of the outflow path for fluid that is constantly being produced in the eye by newly formed blood vessels. This can lead to dangerously high pressures in the eye and is called neovascular glaucoma.
TREATMENT
Systemic Approach to Treat Diabetic Retinopathy
The best treatment for diabetic retinopathy is prevention. Keeping blood sugar levels and blood pressure under control can slow the development or progression of the disease. In most cases, additional ocular treatment is necessary when more advanced complications present, such as macular edema or new blood vessel growth.
Award-winning retinal specialists provide a systemic approach to treating diabetic retinopathy using the newest diagnostic and therapeutic strategies.
Anti-Vasogenic Treatment
Anti-vasogenic injections of the medications Lucentis, Avastin, or Eylea have become the mainstay in controlling retinal edema and have become important adjuncts in treating complications of retinal neovascularization. These drugs stop abnormal blood vessel growth and leakage.
Numerous clinical trials have demonstrated their safety and effectiveness as a treatment for diabetic retinopathy, particularly diabetic macular edema. Treatment consists of fairly regular injections in the first year. Once the retinal situation stabilizes, less frequent injections are necessary. Often, laser treatment will be used to augment and prolong the effect of antivasogenic injections for diabetic macular edema. For proliferative diabetic retinopathy complicated by vitreous hemorrhages, retinal detachment or neovascular glaucoma, laser treatment cannot be replaced by anti-vasogenic treatment, but is rarely done without it now.
Preparation for the injection includes anesthetic and disinfecting eyedrops, placement of a lid speculum to hold the lids open during the injection, and injection of a tiny amount of the medication on the white part of the eye. This is usually minimally uncomfortable, and the actual injection only takes a few seconds. Usually, patients will resume their normal activities the same day.
Laser Surgery
Once diabetic retinopathy is complicated by macular edema or formation of new blood vessels, laser eye surgery for diabetic retinopathy is commonly performed. Lasers have been used to treat diabetic retinopathy for more than 30 years. Treatment is performed in an office setting. During the procedure, green, yellow, red, or infrared laser light is delivered to the retina through the dilated pupil. Typically, a contact lens is placed on the eye, through which the light is transmitted. Topical anesthetic drops are applied for comfort. A local anesthetic may be administered if an extensive amount of laser is needed, or if the patient is very sensitive. Laser surgery is generally used to treat diabetic macular edema and proliferative diabetic retinopathy.
Laser Treatment for Diabetic Macular Edema
The goal of using lasers to treat diabetic macular edema is to stabilize vision by trying to stop damaged blood vessels from leaking fluid into the retina. Compared to those not treated, this can help preserve vision longer. Focal and grid laser surgery are used to treat diabetic macular edema. Focal treatment is effective when there are small areas of leakage. If there are wider areas of leakage, grid laser surgery may be performed, meaning laser spots are transmitted in a grid pattern over the swollen areas of the retina.
Following treatment, small spots may be present in the visual field, which are caused by the laser energy. Eventually, these spots will become less noticeable. The results of laser treatment are not usually immediate. At first vision may get worse, however in the long run, many patients who undergo laser treatment for macular edema do see better. Nowadays, diabetic retinopathy laser treatment is often used in conjunction with intraocular injections.
Intraocular Steroids for Diabetic Macular Edema
Intraocular steroid injections (Triescence, Ozurdex, Kenalog) have not been proven effective across-the-board in clinical trials. However, they have become a standard treatment option for diabetic persons with macular edema who do not respond well to anti-vasogenic or laser treatment alone or in combination. During treatment, a small amount of steroid is injected into the eye using a tiny needle or specialized injection device. The procedure lasts about a minute and is essentially painless.
Side effects include elevated eye pressure and cataracts, which can generally be managed with simple treatments. But more aggressive therapy may be needed.
Laser Treatment for Proliferative Diabetic Retinopathy
The abnormal new blood vessels of proliferative diabetic retinopathy are treated with panretinal (scatter) laser photocoagulation or PRP. During this procedure, the peripheral retina, which is not receiving adequate blood flow, is treated, in order to stop the development of abnormal blood vessels.
This treatment requires many laser applications, and thus may be divided into two or more separate sessions. Treatment stops the formation of new abnormal blood vessels and in most cases causes existing ones to shrink. PRP does not improve vision, but it can prevent the blinding complications of diabetic retinopathy in the majority of cases. Side effects include some loss of peripheral and color vision and a decrease in night vision. Some patients experience blurry vision, which can be temporary or continue indefinitely. Regardless of these side effects, PRP has been shown to decrease the risk of vision loss.
Vitrectomy Surgery for Proliferative Diabetic Retinopathy
Although PRP is often successful in stopping the process of proliferative diabetic retinopathy, in some cases this laser treatment is not effective. Other patients may experience bleeding (vitreous hemorrhage), which makes it impossible for the laser to be delivered to the back of the eye. In most cases, vitreous hemorrhage clears up on its own. However, if it does not clear up after six weeks, a vitrectomy may be necessary. A vitrectomy surgery may also be needed if tractional retinal detachment occurs. In this case, the diabetic retinopathy surgery is performed to stabilize vision and reduce the risk of vision getting worse.
A vitrectomy is a common retinal surgery. During the surgery, vitreous gel is removed using tiny instruments. The surgery is performed in a hospital setting, but on an outpatient basis. If scar tissue has built up on the retina, tiny instruments are utilized to remove the scar tissue. Laser is typically applied to the periphery of the retina during surgery.
During surgery, patients are in a semi-sleep state. The eye is numbed. The surgery lasts about half an hour to three hours, depending on the complexity of the situation. A gas bubble is usually placed inside the eye to serve as an internal “splint” until the retina heals. Over the course of several weeks, the gas bubble is absorbed.
Read more: https://www.vrmny.com/conditions/diabetic-retinopathy/
Vitreous Retina Macula Consultants of New York
950 3rd Ave 3rd floor,
New York, NY 10022
Tel.: (212) 861-9797
Fax.: (212) 628–0698
Web Address https://www.vrmny.com/
Manhattan, NY Office: https://www.vrmny.com/locations/manhattan/
Our location on the map: https://goo.gl/maps/v9rE1BWBd6tsFgPaA
https://plus.codes/87G8Q26J+3R New York
Nearby Locations:
Manhattan, NY
Lenox Hill | Upper East Side | Midtown East | Upper West Side
10021 | 10022 | 10023
Working Hours:
Monday-Friday: 8am–5pm
Payment: cash, check, credit cards.
| Contact This Member | |
| Category | Medical Services |
| View More Details | |
950 3rd Ave 3rd floor, New York, NY 10022, USA
View On Larger Map













Our Network

{kind=link}
Leave Your Comment & Rating Below
0 Comment(s)